Treatment Of Diabetes - Before We Start….
Points to take note are:
Remember Diabetes is an Interplay of ‘Insulin Resistance‘, raising the needs of Insulin and on the other hand “Inability of B cells” to cope up with the demands; together called as Insulin Resistance and Secretory defect ;unless these two happen , Diabetes can not take hold in an individual, therefore, any treatment has to address these two basic problems.
1.)Secretory defects in response to raised demands are best declared by Fasting Blood Glucose levels whereas Insulin resistance causing severely increased demands is best seen as peaking blood glucose levels, in response to a normal or glucose challenge meals.
In Pre-diabetes state both may present separately or together but in a full blown Diabetic both of these are present together ,as a rule
2.) No two patients are same and no single treatment can be exactly workable for two different patients even if they are twins! In other words- No medicine is going to give exactly same effects or side effects in two different individuals.
3.) Every patient passes from different stages of disease and may fluctuate from higher levels to lower and vice versa.
4.) Over the years, Insulin producing B cells in every Pancreas go down in numbers and productivity in fact Diabetes declares on the scene when almost 50% of B cells are either non functional or dead !
Remaining B cells keep losing their Insulin making powers with the passage of time
In fact over 4 to 11 % people or may be more, every year, keep losing B cells completely. At this point you need to have Insulin support from Exogenous sources!
5.) The rate of loss of B cells, though genetically determined, can be slowed for the sure, by Good weight and Diet management at Pre-Diabetes state and when Diabetes sets in, with a good control of Diabetes in addition to these two factors helps in maintaining good health of your B cells.
6.) Also note that in a Diabetic Individual, the mechanisms of slowly Increasing Insulin needs due to Insulin Resistance, after meals or Post- prandial rise in Glucose, followed by B cells “giving up” with Insulin secretion and then secretory capacities going down and down, all happen over the years and all these are stage wise progressions with many modifiable variable like Body weight, Meal size and composition, total calories per day, physical activity and stress, intercurrent diseases and medicines’ intake, are few important ones.
7.) A progressive disease like this ,needs to be matched with progressive and scientific improvisations in the treatment plans; therefore in a single individual at different times and situations we must have different strategies and plans with different Diet, Exercise and Medicinal formulations/combinations and this clearly means a treatment once prescribed ,to successfully control your blood glucose, may not remain efficient for long and sooner or later all this must be redesigned and restructured once again.
Here lies the importance of Regular periodic monitoring and consultations.
8.) Metabolic Memory: Another Important fact-more aggressive you are in maintaining your Glucose levels to near normal, more benefits you will get from the treatment , an early and appropriate control is remembered by the Metabolic system in your body and rewards are sure similarly an undisciplined approach with bad controls in earlier phase ,are also similarly remembered by your system and damage control is less rewarding.
***For all Indian Individuals above 35 yrs of Age it should be mandatory to Test for Fasting Blood Glucose and for Post-Prandial Glucose at TWO hrs after 75 Gs of Glucose load and if found normal then it should be repeated at every 2 yrs!And once the age crosses 40 years ,testing should be annually.
AND Also all overweight(85th percentile weight and above) adolescents of above 10 yrs of age, should be subjected to active screening , because with “soon arriving” puberty and hormonal changes/surges ,this age group will not give you enough time for interventions while progressing from Pre-Diabetes to Diabetes, in fact within few months the damage and progress to Diabetes may be complete and the Intervention phase for Pre-diabetes gets totally missed /lost in the process !
Adolescent Overweight /Obese Children are SPECIAL HIGH RISK CATEGORY:
Moreover an adolescent if develops Diabetes will pose a bigger problem for the society & the family. Let me explain you how. Let us assume that complications take 10 years to develop into the system and another 10 yrs. to cripple you. If Diabetes comes at 15 yrs of age, then by the age of 25 years, when you are getting married and settling down in a job, you start facing the music from Diabetes related complications, for example
you are afraid of facing your wife because of Erection difficulty or getting transient ischemic attack while on Honeymoon! By the age of 35 yrs when your career graph is in full swing, your children are gearing up for higher classes, you are settling down with issues like property ,assets and are consolidating your final positioning in life ,
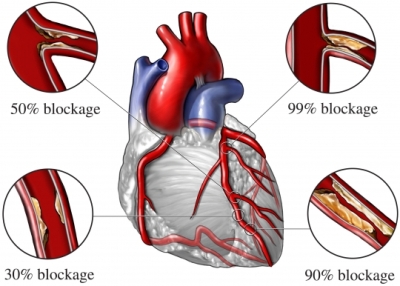
and then suddenly you get your first heart attack! which lands you in ICU ! You may or may not survive or survival thereafter may be just symbolic.
All energies,plans,dreams and ambitions go down the drain !
Just think what kind of life we are giving to our children.
Dear all , I am really very serious about these issues.
Chosing a Drug-Considerations
As we have already pointed in earlier pages that Diabetes Type 1 occurs due to total destruction of Insulin producing B cells and since no insulin is being produced by the body, survival is only possible if enough Insulin is supplied from outside the body.
Insulin Itself Is A Protein And If Taken By Mouth, Our Intestines Will Simply Digest It Like Any Other Protein In Food And No Insulin Will Be Reaching Into The Blood. Therefore, To Ensure That Intact Insulin Reaches Into The Blood Stream It Has To Be Given As Injection.
For Type 1 Diabetes Insulin is the only answer
But in Type 2 Diabetes we have seen that defect is Insufficient OR Inefficient Insulin,for this twin defect state we have some more answers available additional to Insulin.
New Approaches to Managing Diabetes Type 2The convergence of a more complete understanding of the physiologic characteristics of type 2 diabetes with the availability of new therapeutic agents that target the multiple metabolic abnormalities of diabetes has led to new and innovative therapeutic strategies.
In simple terms either you increase the availability of Insulin or make better use of whatever Insulin is available; these two remain the central theme for any treatment plan.
Agents That Target “Insulin Resistance”(NOTE : Weight Reduction, Exercise, Diet planning are the most efficient and cost effective measures and always a part of all treatment plans)
 Oral agents that specifically target insulin resistance include
<>1.The biguanides (metformin) and
Oral agents that specifically target insulin resistance include
<>1.The biguanides (metformin) and
2. TZDs or the thiazolidinediones e.g:. pioglitazone and rosiglitazone.
These agents act on insulin resistance by a different mechanism of action and provide beneficial effects beyond glucose control. Although its mechanism of action is not completely clear, metformin seems to lower fasting blood glucose by improving peripheral insulin sensitivity, reducing hepatic and renal glucose production, and slowing gastrointestinal absorption of glucose.
It does not stimulate insulin secretion or cause Hypoglycemia or weight gain..There is evidence that metformin has beneficial effects on lipids(fats), blood pressure, and pro-coagulant factors associated with the macrovascular morbidities of diabetes.
The thiazolidinediones have been shown to improve glucose control, decrease peripheral insulin resistance, and favorably affect the cardiovascular risk factors of type 2 diabetes (ie, lipid profiles, coagulation and fibrinolysis, and vascular events).
.Their tendency to cause edema(water retention leading to swollen feet)and weight gain-the commonest side-effects, may limit their use in some patients.TZDs ,but with expert hands and vigilant Physician these drugs remain an important tool for glucose control.TZDs as they are also called in short can also be a cause of fractures specially in post-menopausal females i.e.in females after cessation of monthly cycles.
But the biggest problem came after many years of use of Rosiglitazone,which by some researchers was reported to be associated with increased risk of Heart Attacks!For this very reason the drug has now been banned across the globe!
Now we are left with only Pioglitazone which again is being linked to Urinary Bladder Cancers but is being carefully watched!
If used wisely Glitazones are useful drugs. Remember every drug may not suit to everyone!
Agents That "Stimulate Insulin Secretion"-Secretagogues
Sulfonylureas, such as glyburide, glipizide, gliclazide and glimepiride are the agents most commonly used to treat patients with type 2diabetes. Sulfonylureas increase insulin secretion, regardless of the level of circulating glucose.
That’s why if these drugs are taken more then the prescribed dose or a meal is missed or delayed beyond your normal timings you may get abnormal reductions in your Blood Glucose known as Hypoglycemia & SMBG .Which can be potentially life threatening
Glitinides:Two recently introduced short-acting insulinotropic agents, repaglinide and nateglinide, are insulin secretagogues with a relatively shorter onset and duration of action than sulfonylureas.
These agents are specifically indicated to control postprandial glucose excursions and have a low risk for Hypoglycemia & SMBG. Patients are instructed to take these agents before meals, which allows for more flexibility in varying meal patterns without compromising glycemic control.
Agents That Slow Intestinal Absorption of Carbohydrates
The alpha-glucosidase inhibitors, acarbose and miglitol, reduce postprandial glycemia by slowing intestinal glucose absorptionwithout increasing weight gain or the incidence of hypoglycemic events.However, these agents only have a modest effect onreducing blood glucose levels and their use is limited by gastrointestinal side effects.
WHAT IS NEW in Diabetes Treatment

INCRETINS & INCRETIN MIMETICS(Sensible Secretagogues with many more actions !).
Several newly available or emerging treatments in development for people with type 2 diabetes are based on new approaches to treating the disease.
Incretin mimetics are glucagon-like peptide-1 (GLP-1) agonists.GLP-I ia an important product from the Intestines which improves Insulin production and secretion in normal persons and is grossly deficeinet in Diabetics.This hormone improve Beta Cells’ survival also. Exenatide is the one such GLP-1 agonist currently available in India as Byetta is approved by the U.S. Food and Drug Administration (FDA). Another GLP-1 agonist Victoza or liraglutide, which is a GLP-1 analog is once a day therapy and is also available now.Both are Injecctions.first one Twice a day and the second -Once a Day.That means GLP-1 which is deficient in Diabetics,it's action is replicated by these two molecules. Now in normal conditions GLP-1 once produced is destroyed in the body by an enzyme called DPP4 . Therefore the other mean by which you can increase the levels of GLP-1 in Diabetics could be by stopping it's destruction by this enzyme DPP4.Thus came the reason for the development of yet another froup of Drugs-DPP4 Inhibitors.
Dipeptidyl peptidase-IV (DPP-IV) antagonists inhibit the breakdown of GLP-1 by blocking the action of the DPP-IV enzyme and therefore raise GLP-1 (and GIP) levels 2- to 3-fold. These agents have been called incretin enhancers. Sitagliptin was the first of the DPP-IV inhibitors to have received FDA approval.Saxagliptin has now also been apprioved. Sitagliptin,Saxagliptin,Vildagliptin and Linagliptin are FOUR DPP !V inhibitors presently available in India. Other DPP-IV inhibitors are also in development.These will soon arrive in India.Alogliptin is surely going to be with us soon!
Rimonabant was a selective CB-1(cannabinoid-1) receptor blocker,addition of rimonabant to a hypocaloric diet resulted in sustained weight loss and improvements in cardiometabolic risk factors, including waist circumference, high-density lipoprotein (HDL)-cholesterol, triglycerides, glucose and measures of insulin resistance. Rimonabant has been withdrawn (all over the globe) on account of serious Neurological and Psychiatric problems .Research is going on ,however , for safer and better molecules fo CB1 pathway modulation.
Pramlintide, a synthetic analog of another islet hormone, amylin, represents a fifth class of therapy. Pramlintide reduces gastric emptying, suppresses glucagon and enhances satiety, and is FDA-approved for use as an adjunct to meal time insulin in people with type 1 and type 2 diabetes who have failed to achieve glycemic control, despite optimal insulin therapy.
Finally, the first inhaled insulin was recently approved by the FDA.(Has been withdrawn fron market by the company after it’s launch.
Taken together, all of these new therapeutic options -- whether they are available now or in the near future -- have created a new sense of excitement and optimism in the field of diabetes care.
LATEST DRUGS:
Dapagliflozin/Canagliflozin are drugs which will not allow kidneys to hold back Glucose.Whatever Glucose will be filtered out will be allowed to flow into the Urine and will get wasted. Blood Glucose levels will therefore get reduced.In natural conditionsKidneys tend to preserve Glucose.
Bromocriptin and Cloesevelam are two more drugs which I personally find not of much use though have been approved for Diabetes treatment!
There are a few other developments and drugs which are not relevant as far as day to day Diabetes control is concerned.
|MONITORING TARGETS: TREATMENT TARGETS TO BE FIXED ARE:(Non Pregnant Adults)
Fasting Blood Glucose < 110 mg %
And do not care what your lab gives you as normal reference range remember only these above given levels ! At the beginning –Get the following done (Minimum):- Fasting and PP-after meals- Blood Glucose. Afterwards-take time and make a habbit of all the following things:Daily: Weekly : Monthly:
Postprandial at 2H after meals < 140 mg%
Random at any time of the Day < 140 mg%
Yes we are indeed TIGHT on glucose!
HbA1c < 6.5%
Total Cholesterol < 180 mg %
HDL-Cholesterol(Good one) > 40 mg % in males
Triglycerides < 150 mg %
LDL-Cholesterol < 100 mg %
BUT if your patient is fragile,elderly ,living alone, has poor reflexes, already has serious Heart Problems,Cancer or has seriously compromised quality of life,then PLEASE DO NOT TRY TO BE VERY RIGID WITH THE GLUCOSE CONTROLS.Monitoring Your Health and Treatment
Please note that if you are on treatment then glucose has to be tested with your regular dose of medicines and /or Insulin.Because the idea is to see and check how your treatmwent is working for you!
CBC, Kidney Function with Electrolytes, Liver Function Tests, Lipid Profile,HbA1c,Thyroid Function
Test,complete Urine Examination.
->Take your Body weight with minimum of clothes
->Recapitulate what misadventures you did yesterday with meals etc
->Examine your feet(sloes with mirror)
->Have a close look of your teeth, skin, nails, eyes
->Plan your exercise and activity
->Consider your days’ meal plan and provisions for any outdoor meals!
->See that you have adequate and appropriate supply of your medicines
->Make a mental chart of your days’ final schedule!
->Look if any self monitoring is to be done with your glucometer
->Look at your weight chart-identify trends
->Measure your BP
->Look at your blood glucose readings over the past 6-7 days
->Attend to your feet, nails, skin, exercise etc at leisure on your weekly holiday
->Track your doctors’ prescriptions, review your treatment plan, plan your next visit
->Consult your diabetologist
->Get an fasting and PP Blood Glucose done at your neighborhood lab and cross check with your glucometer,
->Check if Lipids,Creatinine,TSH,HbA1c,Urine Protein/Albumin,SGPT/SGPT or any other test in the past which needs to be re-evaluated and revalidated-as per your doctors’ advice