Navigating the Complications: Advanced Organ Protection in 2026
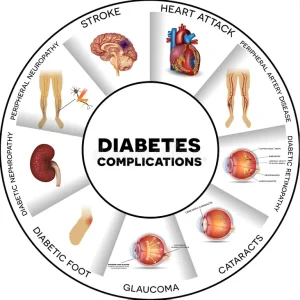
In our “Metabolic Asset Protection” framework, we view complications not as inevitable destinations, but as “mechanical failures” that can be prevented with early detection and the right “maintenance” protocols.
1. Diabetic Nephropathy (Chronic Kidney Disease)
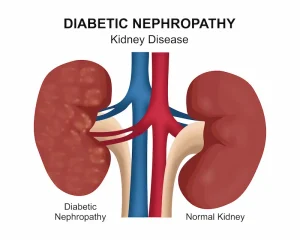
Nephropathy is the progressive damage to the kidney’s filtration units (nephrons) caused by high glucose “friction” and high internal pressure.
The Clinical Brief: High blood sugar damages the delicate micro-vessels in the kidneys, causing them to “leak” protein into the urine (Albuminuria). If left unmanaged, this leads to declining filtration rates (eGFR) and eventual kidney failure.
Guideline-Directed Management (2026):
The Pillars: SGLT2 Inhibitors (e.g., Dapagliflozin) are now mandatory for kidney protection, regardless of glucose levels.
Pressure Control: Mandatory use of ACE Inhibitors or ARBs (RAASi) to reduce internal glomerular pressure.
Targets: Aim for a Urinary Albumin-to-Creatinine Ratio (UACR) < 30 mg/g and stable eGFR.
Monitoring: Annual UACR and serum creatinine tests.
2. Diabetic Neuropathy (Nerve Damage)
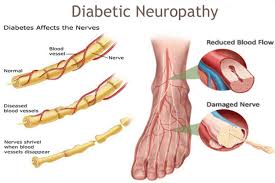
Neuropathy is the most common complication, resulting from metabolic injury to the nerve fibers and the small blood vessels that feed them.
The Clinical Brief: It usually begins as “Peripheral Neuropathy,” affecting the longest nerves first (the feet). Symptoms include tingling, numbness, burning sensations, or a complete loss of feeling. Autonomic Neuropathy can also affect the heart, stomach (gastroparesis), and bladder.
Guideline-Directed Management (2026):
Prevention: Strict glycemic stability to prevent “osmotic swelling” of the nerves.
Symptom Management: Use of Alpha-lipoic acid for nerve repair; Pregalin or Duloxetine for pain.
Advanced Tools: In 2026, we utilize high-frequency vibration testing and monofilament checks to identify “at-risk” nerves before sensation is lost.
Monitoring: Comprehensive foot/nerve exam at every clinical visit.
3. Diabetic Retinopathy (Vision Protection)
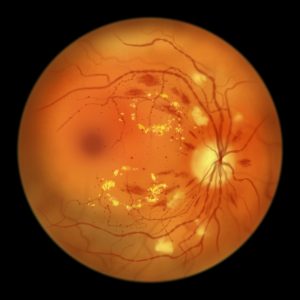
This is a microvascular complication where high glucose weakens the tiny blood vessels in the retina, leading to leakage or the growth of fragile new vessels.
The Clinical Brief: It is often “silent” until vision is affected. It progresses from Non-Proliferative (leaky vessels) to Proliferative (new, weak vessels that can bleed and cause retinal detachment).
Guideline-Directed Management (2026):
Metabolic Control: Tight Blood Pressure (< 130/80) and Glucose control are the only ways to stop progression.
Active Intervention: For advanced stages, Intravitreal Anti-VEGF injections or laser photocoagulation are used to shrink abnormal vessels.
Monitoring: Mandatory Annual Dilated Eye Exam or digital fundus photography starting from the time of Type 2 diagnosis.
4. The Diabetic Foot (The High-Risk Zone)

The “Diabetic Foot” is the result of a “perfect storm”: Neuropathy (can’t feel injury) + Peripheral Arterial Disease (poor blood flow) = Non-healing ulcers and infection.
The Clinical Brief: Small cuts or blisters go unnoticed due to numbness. Because blood flow is poor, the body cannot send “repair crews” (white blood cells and nutrients) to heal the wound, leading to gangrene and potential amputation.
Guideline-Directed Management (2026):
Off-loading: Specialized footwear to remove pressure from ulcers.
Vascular Restoration: Ensuring blood flow via medications or angioplasty if needed.
The Pilot’s Rule: Daily self-inspection using a mirror to check for any redness, swelling, or breaks in the skin.
Professional Care: Regular podiatric debridement and nail care to prevent ingrown toenails or calluses from becoming ulcers.
Dr. Lalwani’s Final Briefing: These complications are the “turbulence” we seek to avoid. By using the Triple Shield (RAASi, Statins, and SGLT2i) and maintaining a strict “Flight Schedule” of screenings, we ensure that these assets—your eyes, your kidneys, and your limbs—stay in service for the duration of your journey.